



HEMP Oil, HEMP SEED oil, and other Unsaturated Fats DANGERS
Attached below is a Ray Peat article about oils in context newsletter (NOT about anything cannabis in his newsletter) in its entirety.
All discussions above Peat’s are based on my own opinions and interpretations and what I have found useful for my own use as well as from feedback from many, many, many, many others.
Follow this link for more information on other Dangerous Items.
I have begun to see CBD and cannabis products advertised using hemp oil, or hemp seed oil as the base.
These are being sold and recommended by otherwise highly influential MDs and highly esteemed virology PhD.s.
Though these providers are highly trained in the current medical and science industries, they perhaps do not have the same understanding of correct physiology and biology in combination with their recommendations. And they also perhaps do not have much cannabis science background.
One particular hemp oil/hemp seed oil line is sold under the guise of Medical Professional Sold only status (similar to a prescription product or Standard Process product, you usually need to talk to a medical provider first, or purchase through a medical provider’s office in order to buy the supplement product).
It’s label says it’s a “full spectrum” product with other cannabis terpenes and compounds. Which is good.
The problem I have with the product shows in the description of ingredients:
“MAX-STRENGTH
6000MG FULL-SPECTRUM CBD
4OZ
“CYTOGENTM Max-Strength Formula is a blend of organic hemp seed oil, organic MCT oil, beta karyophylene and full-spectrum hemp oil. Full spectrum hemp oils cover all the terpenes, flavonoids and phytocannabinoids the plant has to offer. This unique blend is free of additives.”
So here are the problems with these type products, besides just wide-spread fraud about what exactly, and what amounts are even in CBD labeled products.
(There are studies showing over 55% of all cannabis products, particularly CBD cannabis products do not contain what their label states).
First, the oil carrier bases of hemp SEED oil and then “full spectrum hemp oil” and dangerous MCT oil listed in the ingredients as if they were something special. Whatever these oils are actually made of, these oils all, with or without cannabinoids, are highly toxic to ingest in quantity and for long term.
As a note, hemp SEED oil naturally has no cannabinoid compounds in it, and is just another polyunsaturated fatty acid oil (PUFA).
“Full spectrum hemp oil” can only be either hemp SEED oil or some other oil base, such as MCT oil, olive oil, cottonseed oil, some other oil, but with cannabis hemp flower-bud cannabinoids ADDED artificially, like infusing them, back into the oil to make the oil “full spectrum”(containing more cannabinoids than just the CBD molecule).
The CBD is being ADDED to the hemp seed or other base oil in the form of a concentrate, isolate or extraction.

The hemp seed oil as far as I understand is naturally nothing but the (dangerous) base carrier seed or MCT oil. And there otherwise is NO such thing as “hemp oil” if “seed” is not in the name.
Hemp oil does NOT naturally occur and hemp SEED oil does NOT contain any cannabinoid medicine compounds. It only contains seed oil compounds.
For full or broad spectrum hemp oil or hemp seed oil, those cannabinoids need to be ADDED into the recipe of ingredients of the whatever seed or MCT or other carrier oil of the product. This is only a marketing name as “hemp oil” does not exist.
And second, most of these type oil based CBD-only products DO NOT carry enough added CBD (added or natural if there even is any “natural”) to be effective or cost effective.
This advertised product bottle contains a high concentration of cannabinoids into the oil (2000 mg per ounce/30 ML). If taking the 1 ML per day suggested dose, a person is ONLY ingesting 50 mg CBD! Enough to keep you awake at night, but not enough for remedying much else.
See this Wiki article discussing what hemp oil is.
The recommended commercial doses of these type products is often only 25-50 mg of CBD per serving, or even per day, with sometimes 2 or 3 servings a day recommended. The bottle might cost $120 and last a week, a couple weeks.
But the problem with these doses? These very tiny doses of CBD are enough to maybe cause insomnia, but not enough to solve any other problem.
True researchers, like Dr. Bonni Goldstein, MD, suggest the pharmacological CBD mg per day dose needs to be very high like 300-700 mg per dose or per day.
By the way, the dose levels used when part of a CBD prescription for Epidilex®, the FDA approved CBD product to aid in epilepsy, is often 1200- 1500 mg a day.
EPIDIOLEX_cannabidiol_USPI
So with that 30 mg per dose or per day amount, even buying the more expensive bottle of “hemp oil” CBD of 2500 mg in the one ounce, you will get 4 or 5 days out of the bottle if you take the correct amount to help with a malady.
The other problem, discussed more in the CBD section, is that ingesting CBD in large quantities means ingesting it using forms of concentrates, extractions, distillates, isolates combined to meet the dosage on the label.
This is a problem because ingesting CBD (a problem unique to the cannabinoid CBD and not THC) from these excipient isolate products (and hemp seed oil does NOT allow the entourage effect on its own, it has no cannabinoids, CBD or other cannabis compounds in it) usually causes something called a “Bell Curve Effect” that is unique to the individual. This is the unique point in time, and the unique amount dose for an individual consuming a CBD isolate where the CBD stops working.
Isolates-and-Overcoming_the_Bell_Shaped_response_of_CBD
What happens is after a certain amount of ingested isolated CBD, ingested over a certain amount of time, the CBD taken in this form, rather than whole plant form such as a “full spectrum” or “broad spectrum” product, can just stop working as intended.
And no one knows the amount or timing this happens for each individual person. It’s a huge experiment. It’s highly frustrating. And it’s expensive.
High level cannabinoid scientists and researchers, such as Dr. Raphael Mechoulam, PhD., and Dr. Goldstein, have discussed this effect and the quantities needed. Working prescriptions, like Epidilex® took a lot of research to figure out the pharmacological dose for epilepsy.
But these quantities have NOT been researched as much at length to determine other uses and issues the CBD is supposed to be helping.
And often these very large dose quantities come with other side medical side effects.
It has been reported in some of the studies, and even in the Epidilex® product inserts, that consuming these very high pharmacological doses carry additional side effects such as liver toxicity, infections, sleep disorders, fatigue, possibly life-threatening adverse events.
So now the issue is to take a large enough dose of CBD to symptomatically matter vs. taking too much and causing other health issues, vs. taking too little and just having placebo affect at best.
The closest we have to research are the patients Dr. Goldstein has been helping who experimented with the higher 300-700 mg per day and/or per dose quantities and their results. And that she reports on in her book.
AND still, you will BE INGESTING LARGE AMOUNTS OF PUFA causing hemp seed oil!
Hemp seed oil is foremost a seed oil, from hemp SEEDS, with the same seed oil dangers of any of the other seed oils, such as highly harmful seed oil linoleic acids and PUFA (poly unsaturated fatty acids).
Studies pointing out these seed oil compounds, different than the cannabinoid profiles, keep the damaging narrative that seed oils are healthy– they most definitely are NOT. See Peat’s article below and many others from his site about the various oil toxicities.
Again, hemp seed oil contains NO cannabinoids and in my opinion cannot be labeled full or broad spectrum as it is.
And again, hemp oil (without the “seed oil”) is some other base oil, like dangerous MCT oil, or even olive oil, cottonseed oil or even hemp seed oil, but with hemp cannabinoids artificially, or infused, but added back into the oil.
The manufacturer must commercially add other cannabis components besides CBD isolate into the product. If the product ONLY relies on the hemp seed oil, or some base oil NAMED hemp oil because it has hemp CBD added back in for the “spectrum” and only contains isolated CBD plus the hemp seed oil, one is ingesting a CBD isolate, NOT a full or broad spectrum product.
The medicine of the cannabis plant, hemp or marijuana cannabis, is in its sticky resin trichomes on the flower heads (buds) and smaller quantities of the resin on many of the upper leaves and upper stem sections, but not the seeds. The resin has all the cannabinoids like CBD, whatever minimal or not THC, other cannabinoids, terpenes, flavonoids and etc.
And another confusing thing for most sometimes brought up in the discussion– is RSO (Rick Simpson “Oil”).
This RSO is now being sold made out of cannabis hemp plants and sold nationally for concentrated CBD, often in capsule forms.
By the way, I bought some of this CBD RSO and smeared it all over one of my leg varicose veins, covered with a bandage (like Rick Simpson had done with his mix), put some on my face for a skin flap, and ended up with severe burns and eczema on my leg and face from it!
RSO and BHO were among the original concentrates attempts of 20 years ago. They were made by briefly soaking a huge amount of harvested cannabis flower in alcohol or butane and then slow cooking off, at low temps, the alcohol or butane leaving behind an enormously high concentrate of the cannabis trichome resins, with particularly THC concentrated out (something like 900 mg of THC per gram of the sticky goo) along with chlorophyll (making the thick goo dark green) and other cannabinoids that were dissolved in the solvents– and leaving behind an unknown amount of solvent in the mix.
The mixture turned into a dense, thick, sticky semi-gooey sap-like dark liquid that was dispensed through a needle-less catheter syringe often into capsules. This mixture was/is termed “oil”, probably because of the properties of the mix not dissolving readily in water but dissolving better into other “real” oils. There is no oil in this mix, as most would consider oil, no unsaturated or saturated oil in it– perhaps there might be a bit of essential oils of the terpenes in the resin left but often those are so fragile they quickly evaporate off the harvested plant and/or get destroyed in the cooking of the mix.
But making these concentrates the old way often caused enormous damage as those desperate for cures caused massive explosions in its preparation or in its use.
Besides the health consequences of the side effects of enormous-dose THC dosing, without correctly purging all the flammable chemicals out of the final product some people would then light it up (think explode) and try to smoke it.
AND the original RSO mixture in 2003 was used EXTERNALLY to heal the skin cancers of the inventor, Rick Simpson. It wasn’t meant for ingesting at the time.
See the images I took from an antique medical library book I acquired, Remington’s Practice of Pharmacy circa 1907 (Many iterations later, this textbook is still in use in medical schools today, updated to reflect Big Pharma).
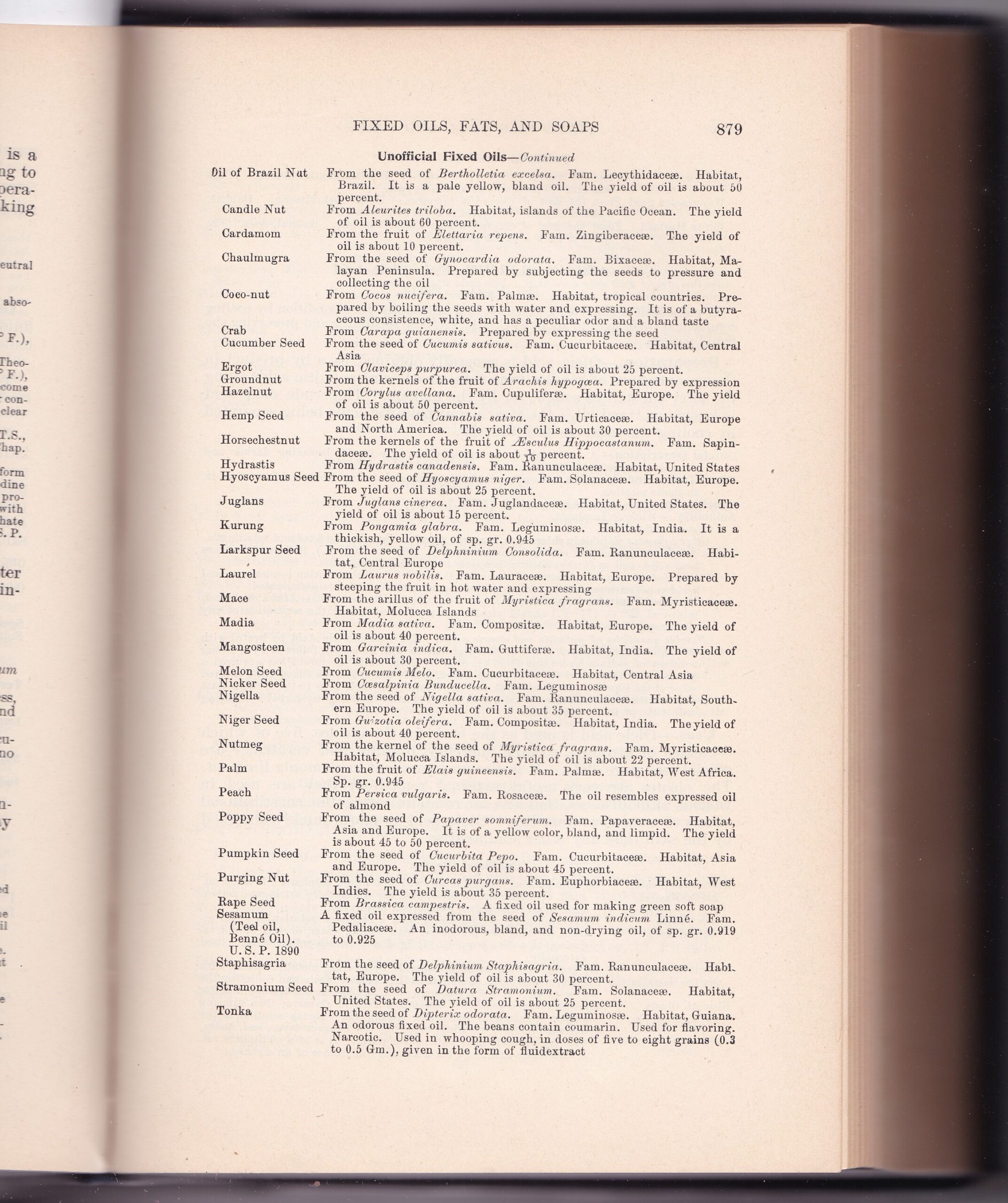
Hemp Seed Oil is under “Unofficial Fixed Oils” with no use specified in a section where other and certain Fixed Oils do list specific uses, many, like cod liver oil, linseed oil, as purgatives and external poultices.
It’s possible it was meant to be eaten, some of the “Unofficial Fixed Oils” I think could be eaten, even coconut oil is listed there. But apparently at the time it was not eaten. There is no mention it contains anything except seed oil and not cannabinoids.
The manual then shows the listings for cannabis and cannabis tinctures. It says “in the powder few or no pollen grains or stone-cells [SEEDS] should be present”.
The tincture is specified to be extracted with alcohol solvent and used as an anodyne [pain reliever] and nervous stimulant [depression, anxiety]. And the dose given varies depending on how the preparation is made and the use.
The powder mentioned was probably ground marijuana cannabis flower powder, and the recipe then was about 3-4 OUNCES (100 gm) ground cannabis flower to eventually 2 pints of alcohol with very specific timings and filterings, and agitations etc.
The dose in 1907 was about 0.3 CC to 0.6 Cc (10 minims) [by my interpretation, about 1/16th to 1/8th of a teaspoon, small doses PRESCRIBED).
Something to remember is that 115 years ago, the cannabis marijuana plant had much weaker concentrations of THC than the hybrids today. I’m thinking no more than 9-10% or maybe less.
And the cannabis hemp plants were used for industrial uses like clothing, rope and a myriad of other non-food, non-medicine uses.
So by my own calculations, assuming 10% THC in the antique marijuana plants and assuming not all the THC was extracted but the mixture was heated at some point before extraction (possibly heated during the grinding stage), one might have 80-90 mg THC to 1 gram of flower. The 2 pints finished liquid using 100 grams of flower it discusses would contain approximately 8000-9000 mg THC. Two pints would contain 1536 doses of 1/8th teaspoon doses of about 4-5 mg THC per dose, about the amount recommended today (using a lot less cannabis for the similar extract today).
So cannabis as medicine, whether preparing THC-rich formulas, or CBD-rich formulas and in line with much of the research documentation suggests using the whole plant flower to make the formulas, not just an isolated compound.
And the better choice is in not using hemp seed oil, or a marketing name of hemp oil to substitute for the whole plant flower, hemp or marijuana, when considering products made as full spectrum or broad spectrum cannabis medicine products.
Here is a PDF of all the cannabis and hemp oil pages from this antique Pharmacy Textbook:
cannabis-hemp-oil-pharmacy-book-cover-all
And Ray Peat’s article, illuminating more about the dangers of seed oils in general:
![]()
A R T I C L E
Oils in Context
An oil researcher[0] spent 100 days eating what he considered to be the “Eskimo diet,” seal blubber and mackerel paste. He observed that his blood lipid peroxides (measured as malondialdehyde, MDA) reached a level 50 times higher than normal, and although MDA is teratogenic, he said he wasn’t worried about fathering deformed children, because his sperm count had gone to zero. Evidently, he didn’t have a very thorough understanding of the Eskimo way of life. In most traditional cultures, the whole animal is used for food, including the brain and the endocrine glands. Since unsaturated fats inhibit thyroid function, and since Eskimos usually have a high caloric intake but are not typically obese, it seems that` their metabolic rate is being promoted by something in their diet, which might also be responsible for protecting them from the effects experienced by the oil researcher. (According to G. W. Crile, the basal metabolic rate of Eskimos was 125% of that of people in the United States.)
People who eat fish heads (or other animal heads) generally consume the thyroid gland, as well as the brain. The brain is the body’s richest source of cholesterol, which, with adequate thyroid hormone and vitamin A, is converted into the steroid hormones pregnenolone, progesterone, and DHEA, in proportion to the quantity circulating in blood in low-density lipoproteins. The brain is also the richest source of these very water-insoluble (hydrophobic) steroid hormones; it has a concentration about 20 times higher than the serum, for example. The active thyroid hormone is also concentrated many-fold in the brain.
DHEA (dehydroepiandrosterone) is known to be low in people who are susceptible to heart disease [1] or cancer, and all three of these steroids have a broad spectrum of protective actions. Thyroid hormone, vitamin A, and cholesterol, which are used to produce the protective steroids, have been found to have a similarly broad range of protective effects, even when used singly. For example, according to MacCallum,
It has been shown that certain lipoid substances, especially cholesterine, can act as inhibiting or neutralizing agents toward such haemolytic poisons as saponin, cobra poison, etc., through forming with them an innocuous compound. Hanes showed that the relative immunity of puppies from chloroform poisoning is due to the large amount of cholesterin esters in their tissues. When artificially introduced into the tissues of adult animals a similar protection is conferred.[2]
A high level of serum cholesterol is practically diagnostic of hypothyroidism, and can be seen as an adaptive attempt to maintain adequate production of the protective steroids. Broda Barnes’ work clearly showed that hypothyroid populations are susceptible to infections, heart disease, and cancer. [3]
In the 1940s, some of the toxic effects of fish oil (such as testicular degeneration, softening of the brain, muscle damage, and spontaneous cancer) were found to result from an induced vitamin E deficiency. Unfortunately, there isn’t much reason to think that just supplementing vitamin E will provide general protection against the unsaturated fats. The half-life of fats in human adipose tissue is about 600 days, meaning that significant amounts of previously consumed oils will still be present up to four years after they have been removed from the diet. [4] According to Draper, et al., [5], , , enrichment of the tissues with highly unsaturated fatty acids results in an increase in lipid peroxidation in vivo even in the presence of normal concentrations of vitamin E. Fasting for more than 24 hours also results in an increase in MDA excretion, implying that lipolysis is associated with peroxidation of the fatty acids released.
According to Lemeshko, et al., it seems that this effect increases with the age of the animal. [6]
Commercial advertising (including medical conferences sponsored by pharmaceutical companies) and commercially sponsored research are creating some false impressions about the role of unsaturated oils in the diet. Like the man who poisoned himself with the “Eskimo diet,” many people focus so intently on avoiding one problem that they create other problems. Since I have discussed the association of unsaturated fats with aging, lipofuscin, and estrogen elsewhere, I will outline some of the other problems associated with the oils, especially as they relate to hormones.
Mechanisms and Essentiality: When something is unavoidable, in ordinary life, talking about “essentiality,” or the minimum amount required for life or for optimal health, is more important as an exploration into the nature of our life than as a practical health issue. For example, how much oxygen, how many germs (of what kinds), how many cosmic rays (of what kinds), would produce the nicest human beings? The fact that we have adapted to something—oxygen at sea level, microbes, or vegetable fats, for example–doesn’t mean that we are normally exposed to it in ideal amounts.
Animals contain desaturase enzymes, and are able to produce specific unsaturated fats (from oleic and palmitoleic acids) when deprived of the ordinary “essential fatty acids,” [7] so it can be assumed that these enzymes have a vital purpose. The high concentration of unsaturated fats in mitochondria–the respiratory organelles where it seems that these lipids present a special danger of destructive oxidation–suggests that they are required for mitochondrial structure, or function, or regulation, or reproduction. Unsaturated fats have special properties of adsorption, [8] and are more soluble in water than are saturated fats. The movement and modulation of proteins and nucleic acids might require these special properties. As the main site of ATP production, I suspect that their water-retaining property might be crucial. When a protein solution (even egg-white) is poured into a high concentration of ATP, it contracts or “superprecipitates.” This condensing, water-expelling property of ATP in protein solutions is similar to the effect of certain concentrations of salts on any polymer. It would seem appropriate to have a substance to oppose this condensing effect, to stimulate swelling [9, 10] and the uptake of precursor substances. Something that has an intrinsic structure-loosening or water-retaining effect would be needed. The ideas of “chaotropic agents” and “structural antioxidants” have been proposed by Vladimirov [11] to bring generality into our understanding of the mitochondria. Lipid peroxides are among the chaotropic agents, and thyroxin is among the structural antioxidants. The known oxygen-sparing effects of progesterone [12, 13] would make it appropriate to include it among the structural antioxidants. The incorporation of the wrong unsaturated fats into mitochondria would be expected to damage the vital respiratory functions.
Some insects that have been studied have been found not to require the essential fatty acids. [14]* According to reviewers, hogs and humans have not been shown to require the “essential” fatty acids. [15] In vitro studies indicate that they are not required for human diploid cells to continue dividing in culture. [16] According to Guarnieri, [17] EFA-deficient animals don’t die from their deficiency. The early studies showing “essentiality” of unsaturated fats, by producing skin problems and an increased metabolic rate, have been criticized [18] in the light of better nutritional information, e.g., pointing out that the diets might have been deficient in vitamin B6 and/or biotin. The similar skin condition produced by vitamin B6 deficiency was found to be improved by adding unsaturated fats to the diet. A fat-free liver extract cured the “EFA deficiency.” I think it would be reasonable to investigate the question of the increased metabolic rate produced by a diet lacking unsaturated fats (which inhibit both thyroid function and protein metabolism) in relation to the biological changes that have been observed. Since diets rich in protein are known to increase the requirement for vitamin B6 [19] (which is a co-factor of transaminases, for example), the increased rate of energy production and improved digestibility of dietary protein on a diet lacking unsaturated fats would certainly make it reasonable to provide the experimental animals with increased amount of other nutrients. With increasing knowledge, the old experiments indicating the “essentiality” of certain oils have lost their ability to convince, and they haven’t been replaced by new and meaningful demonstrations. In the present state of knowledge, I don’t think it would be unreasonable to suggest that the optional dietary level of the “essential fatty acids” might be close to zero, if other dietary factors were also optimized. The practical question, though, has to do with the dietary choices that can be made at the present time.
*If we followed Linus Pauling’s reasoning in determining optimal vitamin C intake, this study of the linoleic acid content of the tissues of an animal which can synthesize it would suggest that we are eating about 100 times more “EFA” than we should.
In evaluating dietary fat, it is too often forgotten that the animals’ diet (and other factors, including temperature) affect the degree of saturation of fats in its tissues, or its milk, or eggs. The fat of wild rabbits or summer-grazing horses, for example, can contain 40% linolenic acid, about the same as linseed oil. Hogs fed soybeans can have fat containing over 30% linoleic acid. [20] Considering that most of our food animals are fed large amounts of grains and soybeans, it isn’t accurate to speak of their fats as “animal fats.” And, considering the vegetable oil contained in our milk, eggs, and meat, it would seem logical to select other foods that are not rich in unsaturated oils.
Temperature and Fat: The fact that saturated fats are dominant in tropical plants and in warm-blooded animals relates to the stability of these oils at high temperatures. Coconut oil which had been stored at room temperature for a year was found to have no measurable rancidity. Since growing coconuts often experience temperatures around 100 degrees Fahrenheit, ordinary room temperature isn’t an oxidative challenge. Fish oil or safflower oil, though, can’t be stored long at room temperature, and at 98 degrees F, the spontaneous oxidation is very fast.
Bacteria vary the kind of fat they synthesize, according to temperature, forming more saturated fats at higher temperatures.[21] The same thing has been observed in seed oil plants. [22] Although sheep have highly saturated fat, the superficial fat near their skin is relatively unsaturated; it would obviously be inconvenient for the sheep if their surface fat hardened in cool weather, when their skin temperature drops considerably. Pigs wearing sweaters were found to have more saturated fat than other pigs.[23] Fish, which often live in water which is only a few degrees above freezing, couldn’t function with hardened fat. At temperatures which are normal for fish, and for seeds which germinate in the cold northern springtime, rancidity of fats isn’t a problem, but rigidity would be.
Unsaturated Fats Are Essentially Involved In Heart Damage: The toxicity of unsaturated oils for the heart is well established, [24, 25, 26] though not well known by the public.
In 1962, it was found that unsaturated fatty acids are directly toxic to mitochondria. [27] Since stress increases the amount of free fatty acids circulating in the blood (as well as lipid peroxides), and since lack of oxygen increases the intracellular concentration of free fatty acids, stored unsaturated fats would seem to represent a special danger to the stressed organism. Meerson and his colleagues [18] have demonstrated that stress liberates even local tissue fats in the heart during stress, and that systematic drug treatment, including antioxidants, can stop the enlargement of stress-induced infarctions. Recently, it was found that the cardiac necrosis caused by unsaturated fats (linolenic acid, in particular) could be prevented by a cocoa butter supplement. [29] The author suggests that this is evidence for the “essentiality” of saturated fats, but points out that animals normally can produce enough saturated fat from dietary carbohydrate or protein, to prevent cardiac necrosis, unless the diet provides too much unsaturated fat. A certain proportion of saturated fat appears to be necessary for stability of the mitochondria. Several other recent studies show that the “essential” fatty acids decrease the P/O ratio, or the phosphorylation efficiency, [30] the amount of usable energy produced by cellular respiration.
There has been some publicity about a certain unsaturated fat, eicosapentaenoic acid, or EPA, which can have some apparently protective and anti-inflammatory effects. A study in which butter was added to the animals’ diet found that serum EPA was elevated by the butter. The investigator pointed out that other studies had been able to show increased serum EPA from an EPA supplement only when the animals had previously been fed butter. [31]
Intense lobbying by the soybean oil industry has created the widespread belief that “tropical oils” cause heart disease. In a comparison of many kinds of oil, including linseed oil, olive oil, whale oil, etc., palm oil appeared to be the most protective. The same researcher [32] more recently studied palm oil’s antithrombotic effect, in relation to platelet aggregation. It was found that platelet aggregation was enhanced by sunflowerseed oil, but that palm oil tended to decrease it.
Much current research has concentrated on the factors involved in arterial clotting. Since the blood moves quickly through the arteries, rapid processes are of most interest to those workers, though some people do remember to think in terms of an equilibrium between formation and removal of clot material. For about 25 years there was interest in the ability of vitamin E to facilitate clot removal, apparently by activating proteolytic enzymes.[33] Unsaturated fats’ ability to inhibit proteolytic enzymes in the blood has occasionally been discussed, but seldom in the U.S. The equilibrium between clotting and clot dissolution is especially important in the veins, where blood moves more slowly, and spends more time.
. . . the slower blood flows the greater its predisposition to clotting. However, this intrinsic process, leading to fibrin production, is slow, taking up to a minute or more to occur. Thrombosis as a result of stasis, therefore, occurs in the venous circulation; typically in the legs where…venous return is slowest. In fact, many thousands of small thrombi are formed each day in the lower body. These pass via the vena cava into the lungs where thrombolysis occurs, this being a normal metabolic function of the organ. [34]
In the Shutes’ research in the 1930s and 1040s, vitamin E and estrogen acted in opposite directions on the clot-removing enzymes.[33] Since estrogen increases blood lipids, and increases the incidence of strokes and heart attacks, it would be interesting to expand the Shutes’ work by considering the degree of saturation of blood lipids in relation to the effects of vitamin E and estrogen on clot removal. Estrogen’s effect on clotting is very complex, since it increases the ratio of unsaturated to saturated fatty acids in the body, and increases the tendency of blood to pool in the large veins, in addition to its direct effects on the clotting factors.
Immunodeficiency and Unsaturated Fats: Intravenous feeding with unsaturated fats is powerfully immunosuppressive [35] (though it often was used to give more calories to cancer patients) and is now advocated as a way to prevent graft rejection. The deadly effect of the long-chain unsaturated fats on the immune system has led to the development of new products containing short and medium-chain saturated fats for intravenous feeding. [36] It was recently reported that the anti-inflammatory effect of n-3 fatty acids (fish oil) might be related to the observed suppression of interleukin-1 and tumor necrosis factor by those fats. [37] The suppression of these anti-tumor immune factors persists after the fish oil treatment is stopped.
As mentioned above, stress and hypoxia can cause cells to take up large amounts of fatty acids. Cortisol’s ability to kill white blood cells (which can be inhibited by extra glucose) is undoubtedly an important part of its immunosuppressive effect, and this killing is mediated by causing the cells to take up unsaturated fats. [38]
Several aspects of the immune system are improved by short-chain saturated fats. Their anti-histamine action [39] is probably important, because of histamine’s immunosuppressive effects.[40] Unsaturated fats have been found to cause degranulation of mast cells.[41] The short-chain fatty acids normally produced by bacteria in the bowel apparently have a local anti-inflammatory action.[42]
A recent discussion of “tissue destruction by neutrophils” mentions “a fascinating series of experiments performed between 1888 and 1906,” in which “German and American scientists established the importance of neutrophil proteinases and plasma antiproteinases in the evolution of tissue damage in vivo.” [43] MacCallum’s Pathology described some related work:
. . . Jobling has shown that the decomposition products of some fats–unsaturated fatty acids and their soaps–have the most decisive inhibiting action upon proteolytic ferments, their power being in a sense proportional to the degree of unsaturation of the fatty acid. So universally is it true that such unsaturated fatty acids can impede the action of proteolytic ferments that many pathological conditions (such as the persistence of caseous tuberculous material in its solid form) can be shown to be due to their presence. If they are rendered impotent by saturation of their unsaturated group with iodine, the proteolysis goes on rapidly and the caseous tubercle or gumma rapidly softens.[44]
Another comment by MacCallum suggests one way in which unsaturated fats could block the action of cytotoxic cells:
This function of the wandering cells is, of course, of immediate importance in connection with their task of cleaning up the injured area to prepare it for repair. While the proteases thus produced are active in the solution of undesirable material, their unbridled action might be detrimental. As a matter of fact, it is shown by Jobling and Petersen that the anti-ferment known to be present in the serum and to restrict the action of the ferment is a recognizable chemical substance, usually a soap or other combination of an unsaturated fatty acid. It is possible to remove or decompose this substance or to saturate the fatty acid with iodine and thus release the ferment to its full activity. [45]
Unsaturated Fats Are Essential For Cancer: The inhibition of proteolytic enzymes by unsaturated fats will act at many sites: digestion of protein, “digestion” of clots, “digestion” of the colloid in the thyroid gland which releases the hormones, the activity of white cells mentioned above, and the normal “digestion” of cytoplasmic proteins involved in maintaining a steady state as new proteins are formed and added to the cytoplasm. It has been suggested that inhibition of the destruction of intracellular proteins would shift the balance toward growth.[46] Cancer cells are known to have a high level of unsaturated fats,[47] yet they have a low level of lipid peroxidation;[48] lipid peroxidation inhibits growth, and is often mentioned as a normal growth restraining factor.[49]
In 1927, it was observed that a diet lacking fats prevented the development of spontaneous tumors.[50] Many subsequent investigators have observed that the unsaturated fats are essential for the development of tumors. [51, 52, 53] Tumors secrete a factor which mobilizes fats from storage, [54] presumably guaranteeing their supply in abundance until the adipose tissues are depleted. Saturated fats–coconut oil and butter, for example–do not promote tumor growth.[55] Olive oil is not a strong tumor promoter, but in some experiments it does have a slightly permissive effect on tumor growth. [56, 57] In some experiments, the carcinogenic action of unsaturated fats could be offset by added thyroid, [57] an observation which might suggest that at least part of the effect of the oil is to inhibit thyroid. Adding cystine to the diet (cysteine, the reduced form of cystine, is a thyroid antagonist) also increases the tumor incidence.[58] In a hyperthyroid state, the ability to quickly oxidize larger amounts of the toxic oils would very likely have a protective effect, preventing storage and subsequent peroxidation, and reducing the oils’ ability to synergize with estrogen.
Consumption of unsaturated fat has been associated with both skin aging and with the sensitivity of the skin to ultraviolet damage, Ultraviolet light-induced skin cancer seems to be mediated by unsaturated fats and lipid peroxidation.[59]
In a detailed study of the carcinogenicity of different quantities of unsaturated fat, Ip, et al., tested levels ranging from 0.5% to 10%, and found that the cancer incidence varied with the amount of “essential oils” in the diet. Some of their graphs make the point very clearly: [52}
This suggests that the optimal EFA intake might be 0.5% or less.
Butter and coconut oil contain significant amounts of the short and medium-chain saturated fatty acids, which are very easily metabolized,[60] inhibit the release of histamine,[39] promote differentiation of cancer cells,[61] tend to counteract the stress-induced proteins,[62] decrease the expression of prolactin receptors, and promote the expression of the T3 (thyroid) receptor. [63] (A defect of the thyroid receptor molecule has been identified as an “oncogene,” responsible for some cancers, as has a defect in the progesterone receptor.)
Besides inhibiting the thyroid gland, the unsaturated fats impair intercellular communication,[64] suppress several immune functions that relate to cancer, and are present at high concentrations in cancer cells, where their antiproteolytic action would be expected to interfere with the proteolytic enzymes and to shift the equilibrium toward growth. In the free fatty acid form, the unsaturated fats are toxic to the mitochondria, but cancer cells are famous for their compensatory glycolysis.
By using lethargic connective tissue cells known to have a very low propensity to take up unsaturated fats [65] as controls in comparison with, e.g., breast cancer cells, with a high affinity for fats, it is possible to show a “selective” toxicity of oils for cancer cells. However, an in vivo test of an alph-linolenic acid ester showed it to have a stimulating effect on breast cancer.[66] Given a choice, skin fibroblasts demonstrate a very specific preference for oleic acid, over a polyunsaturated fat.[67]
Even if unsaturated fats were (contrary to the best evidence) selectively toxic for cancer cells, their use in cancer chemotherapy would have to deal with the issues of their tendency to cause pulmonary embolism,their suppression of immunity including factors specifically involved in cancer resistance, and their carcinogenicity.
Brain Damage And Lipid Peroxidation: When pregnant mice were fed either coconut oil or unsaturated seed oil, the mice that got coconut oil had babies with normal brains and intelligence, but the mice exposed to the unsaturated oil had smaller brains, and had inferior intelligence. In another experiment, radioactively labeled soy oil was given to nursing rats, and it was shown to be massively incorporated into brain cells, and to cause visible structural changes in the cells. In 1980, shortly after this study was published in Europe, the U.S. Department of Agriculture issued a recommendation against the use of soy oil in infant formulas. More recently, [68] pregnant rats and their offspring were given soy lecithin with their food, and the exposed offspring developed sensorimotor defects.
Many other studies have demonstrated that excessive unsaturated dietary fats interfere with learning and behavior, [70, 71] and the fact that some of the effects can be reduced with antioxidants suggests that lipid peroxidation causes some of the damage. Other studies are investigating the involvement of lipid peroxidation in seizures.[72]
The past use of soy oil in artificial milk (and in maternal diets) has probably caused some brain damage. The high incidence of neurological defects (e.g., 90%) that has been found among violent criminals suggests that it might be worthwhile to look for unusual patterns of brain lipids in violent people.
There have been a series of claims that babies’ brains or eyes develop better when their diets are supplemented with certain unsaturated oils, based on the idea that diets may be deficient in certain types of oil, Some experimenters claim that the supplements have improved the mental development of babies, but other researchers find that the supplemented babies have poorer mental development. But the oils that are added to the babies’ diets are derived from fish or algae, and contain a great variety of substances (such as vitamins) other than the unsaturated fatty acids, and the researchers consistently fail to control for the effects of such substances.
It has shown that it is probably impossible to experience a detectable deficiency of linoleic acid outside of the laboratory setting,[69] but the real issue is probably whether the amount in the normal diet is harmful to development. Until the research with animals has produced a better understanding of the effects of unsaturated oils, experimenting on human babies seems hard to justify.
Marion Diamond, who has studied the improved brain growth in rats given a stimulating environment (which, like prenatal progesterone, produced improved intelligence and larger brains), observed that in old age the “enriched” rats’ brains contained less lipofuscin (age pigment).[73] It is generally agreed that the unsaturated oils promote the formation of age pigment. The discovery that stress or additional cortisone (which, by blocking the use of glucose, forces cells to take up more fat) causes accelerated aging of the brain[74] should provide new motivation to investigate the antistress properties of substances such as the protective steroids mentioned above, and the short-chain saturated fats.
Essential for Liver Damage: Both experimental and epidemiological studies have shown that dietary linoleic acid is required for the development of alcoholic liver damage.[75] Animals fed tallow and ethanol had no liver injury, but even 0.7% or 2.5% linoleic acid with ethanol caused fatty liver, necrosis, and inflammation. Dietary cholesterol at a level of 2% was found to cause no harm,[76] but omitting it entirely from the diet caused leakage of amino-transferase enzymes. This effect of the absence of cholesterol was very similar to the effects of the presence of linoleic acid with ethanol.
Obesity: For many years studies have been demonstrating that dietary coconut oil causes decreased fat synthesis and storage, when compared with diets containing unsaturated fats. More recently, this effect has been discussed as a possible treatment for obesity.[77] The short-chain fats in coconut oil probably improve tissue response to the thyroid hormone (T3), and its low content of unsaturated fats might allow a more nearly optimal function of the thyroid gland and of mitochondria. A survey of other tropical fruits’ content of short and medium chain fatty acids might be useful, to find lower calorie foods which contain significant amounts of the shorter-chain fats.
Other Problem Areas: The presence of palmitate in the lung surfactant phospholipids[78] suggests that maternal overload with unsaturated fats might interfere with the formation of these important substances, causing breathing problems in the newborn. The bone-calcium mobilizing effect of prostaglandins suggests that dietary fats might affect osteoporosis; the absence of osteoporosis in some tropical populations might relate to their consumption of coconut oil and other saturated tropical oils. The steroids which occur in association with some seed oils might be nutritionally significant, in the way animal hormones in foods undoubtedly are. For example, soy steroids can be converted by bowel bacteria into estrogens. R. Marker, et al., found diosgenin (the material in the Mexican yam from which progesterone, etc., are derived) in a palm kernel, Balanites aegyptica (Wall).[79] Another palm fruit also contains sterols with anti-androgenic and anti-edematous actions.[80, 81]
If the amount of ingested unsaturated fats (inhibitors of protein digestion) were lower, protein requirements might be lower.
The similar effects of estrogen and of polyunsaturated fats (PUFA) are numerous. They include antagonism to vitamin E and thyroid, to respiration and proteolysis; promotion of lipofuscin formation and of clot formation, promotion of seizure activity, impairment of brain development and learning; and involvement in positive or negative regulation of cell division, depending on cell type.
These parallels suggest that the role of PUFA in reproduction might be similar to that of estrogen, namely, the promotion of uterine and breast cell proliferation, water uptake, etc. Such parallels should be a caution in generalizing from the conditions which are essential for reproduction to the conditions which are compatible with full development and full functional capacity. If a certain small amount of dietary PUFA is essential for reproduction, but for no other life function, then it is analogous to the brief “estrogen surge,” which must quickly be balanced by opposing hormones. The present approach to contraception through estrogen-induced miscarriage might give way to fertility regulation by diet. A self-actualizing pro-longevity diet, low in PUFA, might prolong our characteristically human condition of delayed reproductive maturity, and, if PUFA are really essential for reproduction, unsaturated vegetable oils could temporarily be added to the diet when reproduction is desired.
Conclusions: Polyunsaturated fats are nearly ubiquitous, but if they are “essential nutrients,” in the way vitamin A, or lysine, is essential, that has not been demonstrated. It seems clear that they are essential for cancer, and that they have other properties which cause them to be toxic at certain levels. It might be time to direct research toward determining whether there is a threshold of toxicity, or whether they are, like ionizing radiation, toxic at any level.
Note:
A possible mitochondrial site for toxicity: In 1971 I was trying to combine some of the ideas of Albert Szent-Gyorgyi, Otto Warburg, W. F. Koch, and L. C. Strong. I was interested in the role of ubiquinone in mitochondrial respiration. In one experiment, I was using paper chromatography to compare oils that I had extracted from liver with vitamin E and with commercially purified ubiquinone. Besides using the pure substances, I decided to combine vitamin E with ubiquinone for another test spot. As soon as I combined the two oils, their amber and orange colors turned to an inky, greenish black color. I tested both bacterial and mammalian ubiquinone, and benzoquinone, and they all produced similar colors with vitamin E. When I ran the solvent up the paper, the vitamin E and the ubiquinone traveled at slightly different speeds. The black spot, containing the mixture, also moved, but each substance moved at its own speed, and as the materials separated, their original lighter colors reappeared. Charge-transfer bonds, which characteristically produce dark colors, are very weak bonds. I think this must have been that kind of bond. Years later, I tried to repeat the experiment, using “ubiquinone” from various capsules that were sold for medical use. Instead of the waxy yellow-orange material I had used before, these capsules contained a liquid oil with a somewhat yellow color. Very likely, the ubiquinone was dissolved in vegetable oil. At the time, I was puzzled that the color reaction didn’t occur, but later I realized that a solvent containing double bonds (e.g., soy oil or other oil containing PUFA) would very likely prevent the close association between vitamin E and ubiquinone which is necessary for charge-transfer to occur. Since I think Koch and Szent-Gyorgyi were right in believing that electronic activation is the most important feature of the living state, I think the very specific electronic interaction between vitamin E and ubiquinone must play an important role in the respiratory function of ubiquinone. Ubiquinone is known to be a part of the electron transport chain which can leak electrons, so this might be one of the ways in which vitamin E can prevent the formation of toxic free-radicals. If it can prevent the “leakage” of electrons, then this in itself would improve respiratory efficiency. If unsaturated oils interfere with this very specific but delicate bond, then this could explain, at least partly, their toxicity for mitochondria. [“Electron leak” reference: B. Halliwell, in Age Pigments (R. S. Sohal, ed.), pp. 1-62, Elsevier, Amsterdam, 1981.]
REFERENCES
- Sinclair, H., Prog. Lipid Res. 25: 667-72, “History of EFA & their prostanoids: some personal reminiscences.”
- E. Barrett-Connor, N. Engl. J. Med., Dec. 11, 1986, and R. D. Bulbrook (London Imperial Cancer Research Fund, discussed in a review by H. G. Schwartz.
- MacCallum, W. G., A Text-Book of Pathology, W. B. Saunders Co., Phila., 1937, pp. 85-86.
- Barnes, Broda, and L. Galton, Hypothyroidism: The Unsuspected Illness, T. Y. Crowell, New York, 1976.
- Beynen, A. C., P. J. J. Hermus, and J. G. A. J. Hautvast, “A mathematical relationship between the fatty acid composition of the diet and that of the adipose tissue in man,” Am. J. Clin. Nutr. 33(1), 81-5, 1980.
- Draper, H. H., et al., Lipids 21(4), 305-7, 1986, “Metabolism of MDA.”
- Lemeshko, V. V., et al., Uk. Biokhim. Zh. 54(3), 325-7, 1982.
- Guarnieri, M., “The essential fatty acids,” Adv. Lip. Res. 8, 115, 1970.
- Ibid., p. 163.
- Abuirmeileh, N. M., “The effect of dietary fats on liver mitochondrial fatty acid profiles in the rat,” Dirasat (Ser.): Nat. Sci. (Univ. Jordan) 7(2), 51-7, 1980.
- Marcus, A. J., “Role of lipids in blood coagulation,” Adv. Lip. Res. 4, 1-38, 1966, citation of Trojan and Johnson, 1968.
- Vladimirov, Yu. A., “Lipid peroxidation in mitochondrial membrane,” Adv. Lip. Res.7, 173-249, 1980.
- Diamond, M., Enriching Heredity, Free Press, 1988, p. 131.
- Duval, D., S. Durant, and F. Homo-DeLarche, “Non-genomic effects of steroids,” B.B.A. 737 409-42, 1983 (p. 426).
- Rapport, E. W., et al., “Ten generations of Drosophila melanogaster reared axenically on a fatty acid free holidic diet.” Arch. Insect Biochem. 1(3), 243-250, 1984.
- Deuel, H. J., and R. Reiser, “Physiology and biochemistry of the essential fatty acids,” Vitamins and Hormones 13, 1-70, 1955 (p. 50).
- Bettger, W. J., and R. G. Ham, “Effects of non-steroidal anti-inflammatory agents and anti-oxidants on the clonal growth of human diploid fibroblasts,” Prog. Lipid Res. 20, 265-8, 1981.
- Guarnieri, p. 115.
- McHenry, E. W., and M. L. Cornett, “The role of vitamins in anabolism of fats,” Vitamins and Hormones 2, 1-27, 1944.
- Canham, J. E., et al., “Dietary protein–its relationship to vitamin B6 requirements and function,” Ann. N. Y. Acad. Sci. 166, 1629, 1969.
- Ellis and Isbell, cited in McHenry and Cornell, p. 23.
- Terroine, E. F., et al., “Sur le signification physiologique des liaisons ethyleniques des acides gras,” Bull. Soc. Chim. Biol. 9(5), 605-20, 1927.
- Wolf, R. B., “Effect of temperature on soybean seed constituents,” J. Am. Oil Chem. Soc. 59(5) 230-2, 1982.
- Prof. Ray Wolfe, “Chemistry of nutrients and world food,” Univ. of Ore. Chem. 121, October 16, 1986.
- Selye, H., “Sensitization by corn oil for the production of cardiac necrosis,” Amer. J. of Cardiology 23, 719-22, 1969.
- Byster, G. and R. Vles, “Nutritional effects of rapeseed oils in pigs. 3. Histometry of myocardial changes,” Proc. Int. Rapeseed Conf., 5th, 1978 (publ. 1979) 2, 92-4.
- Roine, P., E. Uksila, H. Teir, and J. Rapola, Z. Ernahrungsw. 1, 118-124, 1960.
- Borst, P., J. A. Loos, E. J. Christ, and E.C. Slater, “Uncoupling action of long chain fatty acids,” Biochem. Bioph. Acta 62, 509-18, 1962.
- Kramer, J. K. G., E. R. Farnworth, B. K. Thompson, A. H. Corner, and H. L. Trenholm, “Reduction of myocardial necrosis in male albino rats by manipulation of dietary fatty acid levels,” Lipids 17(5), 372-82, 1982.
- Meerson, F. Z., et al., Kardiologiya 9, 85, 1982, and Kagan, V. E. Kagan, et al., “Calcium and lipid peroxidation in mitochondrial and microsomal membranes of the heart,” Bull. Exp. Biol. And Med. 95(4), 46-48, 1983.
- Rapoport, S., and T. Schewe, “Endogenous inhibitors of the respiratory chain, Trends in Biochem. Scis., Aug., 1977, 186-9, and Abuirmeileh, N. M., and C. E. Nelson, “The influence of linoleic acid intake on electron transport system somponents,” Lipids 15, 925-31, 1980.
- O’Dea, K., M. Steel, J. Naughton, A. Sinclair, G. Hopkins, J. Angus, Guo-Wei He, M. Niall, and T. J. Martin, “Butter-enriched diets reduce arterial prostacyclin production in rats,” Lipids 23(3), 234-40, 1988.
- Rand, M. L., et al., “Dietary palmitate and thrombosis,” Lipids 23(11), 1988, and Hornstra, G., “Arterial thrombus formation in rats,” in Biological Effects of Fats.
- Shute, W. E., and H. J. Taub, Vitamin E for Ailing and Healthy Hearts, Pyramid House Books, New York, 1969, p. 191.
- Max, B., “Clots and Creamers,” Trends in Pharmacological Scies. 9(4), 122-4, 1988.
- Mascioll, E. A., et al., “Medium chain triglycerides and structured lipids as unique nonglucose energy sources in hyperalimentation,” Lipids 22(6) 421-3, 1987.
- Hashimn, S. A., and P. Tantibhedyangkul, “Medium chain triglycerides in early life: effects on growth of adipose tissue,” Lipids 22(6), 429-34, 1987.
- Endres, S., et al., “The effect of dietary supplementation with n-3 polyunsaturated fatty acids on the synthesis of interleukin-1 and tumor necrosis factor by mononuclear cells,” N. Engl. J. Med. 320(5), 265-71, 1989 (Feb. 2).
- Meade, C.J., and J. Martin, Adv. Lipid Res. 1978, 127-185.
- Brockelhurst, W. E., Pharmacological mediators of hypersensitivity reactions, in Clinical Aspects of Immunology (P. G. H. Gell and R. R. A. Coombs, editors) Blackwell Scientific, P. A. Davis Co., Phil., 1963, p. 360.
- Axhnaper, H. W., T. M. aune, and R. K. Roby, “A role for histamine type II (H-2) binding in productin of the lymphokine, Soluble Immune Response Suppressor (SIRS),” J. Immun. 1391, 1185, 1987.
- Guillosson, J. J., C. Piette, and M. Piette, “Disparity of in vitro behaior of mastocytes under the effects of two lipid suspensions differing by their content in unsaturated fatty acids,” Ann. Pharm. Fr. 37(1-2), 27-32, 1979.
- Harig, J. M., et al., “Treatment of diversion colitis with short-chain-fatty acid irrigation,” N. Engl. J. Med. 320(1), 23-8, 1989.
- Weiss, S. J., “Tissue destruction by neutrophils,” N. Engl. J. Med. 320(6), 365-76, 1989.
- MacCallum, op. Cit. P. 85.
- Ibid., p. 162.
- Yucel, t., J. Ahlberg, and H. Glauman, “Overall proteolysis in perfused and subfractionated chemically induced malignant hepatoma of rat: effects of amino acids,” Exp. And Mol. Path. 50, 38-49, 1989.
- Lankin, V. Z., and E. A. Neifakh, Izv. Akad. Nauk SSR, Ser. Biol. 2, 263. : Izv Akad Nauk SSSR Biol 1968 Mar-Apr;2:263-8 [Higher fatty acids in the process of malignant growth].[Article in Russian]
- Neifakh, E. A., and Kagen, V. E., Biokhimiya 34, 511, 1969; Slater, T. F., “Lipid peroxidation,” Biochem. Soc. Trans. 10: 70-71, 1982.
- Burlakova EB, Molochkina E. M., Pal’mina N. P., “Role of membrane lipid oxidation in control of enzymatic activity in normal and cancer cells,” Adv Enzyme Regul 1980;18:163-79; Duchesne, J., “Le fonction immunologique et le cancer,” Ann. Biol. XVI95-6), 271-6, 1977; Vladimirov, Yu. A., “Lipid peroxidation in mitochondria,” Adv. Lipid Res. 7, 173-249, 1980.
- Bernstein, S. and H. Elias, “Lipoids and carcinoma growth,” Zeitschr. Krebsforsh. 28(1), 1-14, 1927.
- Jurkowski, J. J., et al., J. Natl. Can. Inst. 74(5), 1135-50, 1985.
- Ip, C., et al., “Requirement of essential fatty acids for mammary tumor,” Cancer Res. 45(5), 1997-2001, 1985.
- Xohwn, L. .et al., Cancer Res. 44(11), 5023-38, 1984.
- Kitada, S., E. F. Hays, and J. F. Mead, “A lipid mobilizing factor in serum of tumor-bearing mice,” Lipids 15(3), 168-74.
- Cohen, L. A. and D. O. Thompson, “The influence of dietary medium chain triglycerides on rat mammary tumor development,” Lipids 22(6), 455-61, 1987; Miller, J. A., et al., “Carcinogenicity of p-dimethylaminoazobenzene in diets containing hydrogenated coconut oil,” Cancer Res. 4, 153-8, 1944.
- Tinsley I. J., et al., “Tissue fatty acid changes and tumor incidence in C3H mice ingesting cottonseed oil,” Lipids 1982 Feb;17(2):115-7.
- Benson, J., M. Lev, and C. G. Grand, “Enhancement of mammary fibroadenoma in female rat by a high fat diet,” Cancer Res. 16, 137, 1956.
- Tannenbaum, A., and H. Silverstone, “Effects of varying proportion of protein in the diet,” Cancer Res. 9, 162, 1949.
- Black, H. S., W. A. Lenger, J. Gerguis, and J. I. Thornby, “Relation of antioxidants and level of dietary lipids to epidermal lipid peroxidation and ultraviolet carcinogenesis,” Cancer Res. 45(12, pt 1), 6254-9, 1985.
- Babayan, V. K., “Medium chain triglycerides and structured lipids,” Lipids 22, 417-20, 1987.
- Prasad, K. N., “Minireview: butyric aicd,” Life Science 27, 1351-8, 1980.
- Rousseau, G. G., “Control of gene expression by glucocorticoid hormones,” Biochem. J. 224, 1-12, 1984.
- Ortiz-Caro J, F. Montiel, A. Pascual, A. Aranda, “Modulation of thyroid hormone nuclear receptors by short-chain fatty acids in glial C6 cells. Role of histone acetylation,” J Biol Chem 1986 Oct 25;261(30):13997-4004.
- Aylsworth, C. F., C. W. Welsch, J. J. Kabora, and J. E. Trosko, “Effect of fatty acids on junctional communication: possible role in tumor promotion by dietary fat,” Lipids 22(6), 445-54, 1987.
- Lynch, R. D., “Utilization of polyunsaturated fatty acids by human diploid cells aging in vitro,” Lipids 15(6_, 412-20, 1980.
- Kudryavtsev, I. A., et al., “Character of the modifying action of polyunsaturated fatty acids on growth of transplantable tumors of various types,” Bull. Exp. Biol. And Med. 105(4), 567-70, 1988.
- Rosenthal, M. D., “Selectivity of incorporation, utilization and retention of oleic and linoleic acids by human skin fibroblasts,” Lipids 15(10), 838-47, 1967.
- Bell, J. M. and P. K. Lundberg, “Effects of a commercial soy lecithin preparation on development of sensorimotor behavior and brain biochemicals in the rat,” Dev. Psychobiol. 8(1), 59-66, 1985.
- Martinez, M., and A. Ballabriga, “Effects of parenteral nutrition with high doses of linoleate on the developing human liver and brain,” Lipids 22(3), 133-6, 1987.
- Harman, D., et al., “Free radical theory of aging: effect of dietary fat on central nervous system function,” J. American Geriatrics Soc. 24(1) 292-8, 1976; Eddy, D. E., and D. Harman, “Rat brain fatty acid composition: effect of dietary fat and age,” J. Gerontol. 30(6), 647-54, 1975; Harman, D., “Lipofuscin and ceroid formation: the cellular recycling system,” Adv Exp Med Biol 266:3-15, 1989.
- Meerson, F. Z., et al., “Effect of the antioxidant ionol on formation and persistence of a defensive conditioned reflex during peak exercise,” Bull. Exp. Biol. Med. 96(9), 70-71, 1983.
- Kryzhanovskii, G. N., E. V. Nikushkin, I. R. Tupeav, and V. E. Braslavski, “Anticonvulsant action of superoxide dismutase,” Bull. Exp. Biol. And Med. 103(4), 444-6, 1987.
- Diamond, M., Enriching Heredity, Free Press, New York, 1988, p. 146.
- Sapolsky, R. M., L. C. Krey, and B. S. McEwen, “Neuroendrocrinology of stress and aging: the glucorticoid cascade hypothesis,” Endocr. Revs. 7(3), 284-301, 1986.
- Nanji, A. A., and S. W. French, “Dietary linoleic acid is required for development of experimentally induced alcoholic liver-injury,” Life Sciences 44, 223-301, 1989.
- Laitinen, M., et al., “Effects of dietary cholesterol feeding on the membranes of liver cells and on the cholesterol metabolism in the rat,” Int. J. Bioch. 14(3), 239-41, 1982.
- Ling, P., et al., “Evaluation of protein quality of diets containing medium and long chain triglycerides in healthy rats,” J. Nutrition 116, 343-8, 1986.
- Sato, T. and T. Akino, “Source of lung surfactant phospholipids: Comparison of palmitate and acetate as precursors,” Lipids 17(12), 884-92, 1982.
- Marker, R. E., et al., “The steroidal sapogenin from Balanites aegyptica (Wall),” J. Amer. Chem. Soc. 65(6), 1943.
- Tarayre, J. P. et al., [Anti-edematous action of a hexane extract of the stone fruit of Serenoa repens Bartr], Ann. Pharm. Fr. 41, 550-70, 1983.
- Champault, G., et al., “A double-blind trial of an extract of the plant Serenoa repens in benign prostatic hyperplasia,” Br. J. Clin. Pharmacol. 18, 461-2, 1984.
© Ray Peat 2006. All Rights Reserved. www.RayPeat.com